Cholesterol and Everything You Should Know – Part 1
A plain-language primer on cholesterol and lipidology — what LDL, HDL, and apoB really mean, and why "high cholesterol" is not the whole story.
My deep dive into lipidology and cholesterol began during my first year of Preventive Medicine residency.
Here, I’ll take this approach: simple without being simplistic. In a way, that you should be equipped well enough to read new studies and evidence on your own.
For the newest guidelines: please check the National Lipid Association and American Heart Association
Let’s get started.
Table of Contents
What is Cholesterol
Cholesterol is an organic molecule that our body needs to build cell membranes (every single cell), to make hormones, vitamin D, and bile acids. It is present in all animals and our liver and cells makes most of the circulating cholesterol. Yes, most of it does not come from the diet.
What is the role of diet
As I mentioned, our liver makes most of the circulating cholesterol. The amount you eat has to be unpacked and travel across the gut wall cells (enterocytes) before it can matter.
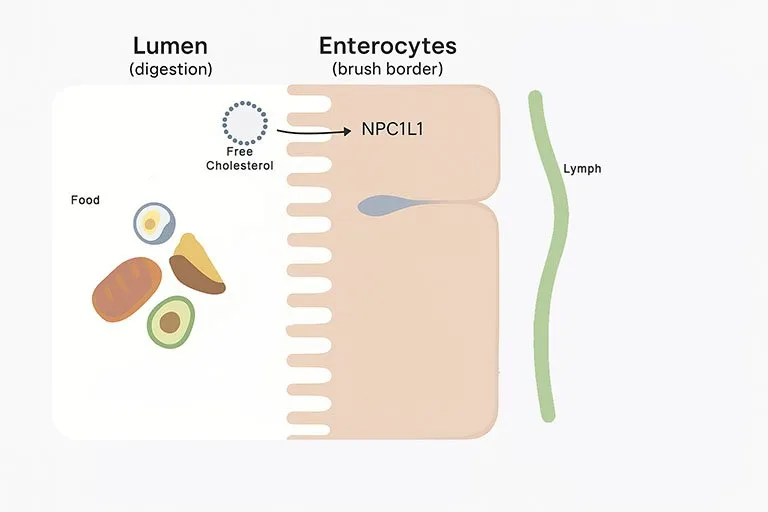
In the intestinal lumen
Bile salts dissolve cholesterol into tiny micelles; pancreatic enzymes first convert any cholesteryl esters in food into free (unesterified) cholesterol.
In the intestinal cells
That free cholesterol is then pulled into the gut cell by a gateway protein called NPC1L1. From there, newly discovered Aster proteins move that cholesterol inside the cell to the endoplasmic reticulum, where it’s re-esterified by ACAT2 and packed into chylomicrons that enter the lymph and then the bloodstream.
Kicking some cholesterol back into the lumen
Done! That’s how you absorb the cholesterol from your diet. However, the body also has a built-in brake: ABCG5/8 pumps some sterols back into the gut, so not everything you eat gets through. Therefore, if the body understands that it has too much cholesterol, it is going to kick out the excess.
What is Bile, Unesterified and Sterified Cholesterol
PS.: If you go back to the cholesterol molecule, the red oxygen atom is the exact position that a fatty acid would bind to make and ester.
Now, speaking of bile, we must understand what it is. Bile is a fluid made of bile acids, phospholipids, cholesterol, and other compounds. When we eat, the gallbladder releases bile into the intestine to help digest fats.
Bile acids break large fat droplets into tiny micelles that allow cholesterol and fat to dissolve in the watery environment of the gut. Only free (unesterified) cholesterol—that is, cholesterol not bound to a fatty acid—can pass through the intestinal wall. Most cholesterol in food, however, is in the esterified form (cholesteryl esters), meaning a fatty acid is attached to it. These esters must first be de-esterified (broken back into the free form) by pancreatic cholesterol esterase before absorption is even possible.
Even then, absorption is not guaranteed. Some cholesterol never makes it into micelles; some is pumped back out by ABCG5/ABCG8 transporters; and the main gatekeeper, NPC1L1, can be down- or up-regulated depending on your body’s needs.
The interesting part is that most of the cholesterol inside your intestine isn’t from your diet at all—it’s from your own liver. The liver secretes cholesterol into bile mostly in its free form, not as an ester, so it has a much easier path through the intestinal wall.
In summary so far: the cholesterol that comes from food is mostly in the esterified form and must first be “broken down” to its free form (unesterified) before it can be absorbed, while cholesterol secreted in bile is already in its free form.
All good? Then…
After bile acids and cholesterol finish their job, about 95% are reabsorbed in the small intestine and sent back to the liver through the enterohepatic circulation. The small fraction that isn’t reabsorbed is excreted in the stool. That’s one of the main natural routes for getting rid of cholesterol.
The liver replaces those lost bile acids by converting more cholesterol into new bile acids, through an enzyme called CYP7A1. This feedback system keeps your cholesterol levels in balance — and it’s the same loop targeted by medications like ezetimibe and bile acid sequestrants, which reduce cholesterol by interrupting this recycling process.
People absorb very different amounts
You can probably already see, based on how many steps and variables there are, why humans vary widely in fractional cholesterol absorption—ranging from less than 20% to more than 80%. Because of differences in transporter expression, bile acid pools, microbiome, and genetics.
Variants in genes like ABCG5/8, NPC1L1, APOE, MTTP, LDLR and others help explain why some people are “hyper-responders” to dietary cholesterol while most are not.
In controlled feeding data, ~15–25% are hyper-responders; a standard 100-mg/day increase in dietary cholesterol can raise LDL-C several-fold more in them than in hypo-responders. This is why two people can eat the same food and see very different lab changes.
It’s very important to understand that there is still a lot we don’t know about the exact mechanistic pathways of cholesterol. The summary is that saturated fat in the diet often increases the cholesterol particles responsible for heart attacks and stroke when compared to cholesterol in the diet.
What diet changes move cholesterol the most (and why)
We haven’t talked about LDL, apo B, or lipoproteins yet. But we’ll get there in the next part of the series.
For now, you should know that for most people, the type of fat you eat is the biggest dietary driver of LDL/apoB (considered harmful molecules or “bad cholesterol”)—not the cholesterol content of individual foods. Replacing saturated fat (found in fatty meats, butter, full-fat dairy, many baked goods) with unsaturated fats (olive oil, nuts, seeds, fish, other plant oils) lowers LDL and apoB and, in longer trials, reduces cardiovascular events.
This pattern has been consistent across metabolic ward studies, randomized trials, and modern guidance.
Saturated fat vs Unsaturated fat
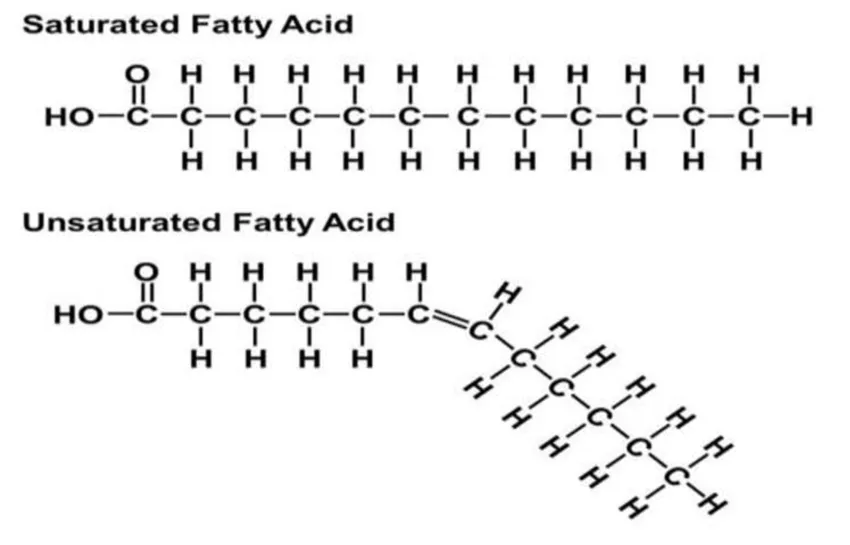
When people refer to saturated or unsaturated fat, they usually mean triglycerides (the fats in our diet and body) in which the fatty acid chains are “saturated” or “unsaturated”.
Saturated fatty acids are have no double bonds, which means that they are saturated with hydrogen atoms and do not have space for more. Therefore they are more stable, strong, with straight-lined molecules, and solid in room temperature.
Unsaturated fatty acids have double bonds between carbons. Meaning that they still have space for more hydrogen atoms. In room temperature they are oils. And by the way, these extra hydrogen atoms can be added by hydrogenating these unsaturated fats and transforming them into saturated fat under specific conditions that can be achieved in a lab.
Monounsaturated = one double bond.
Polyunsaturated = two or more double bonds.
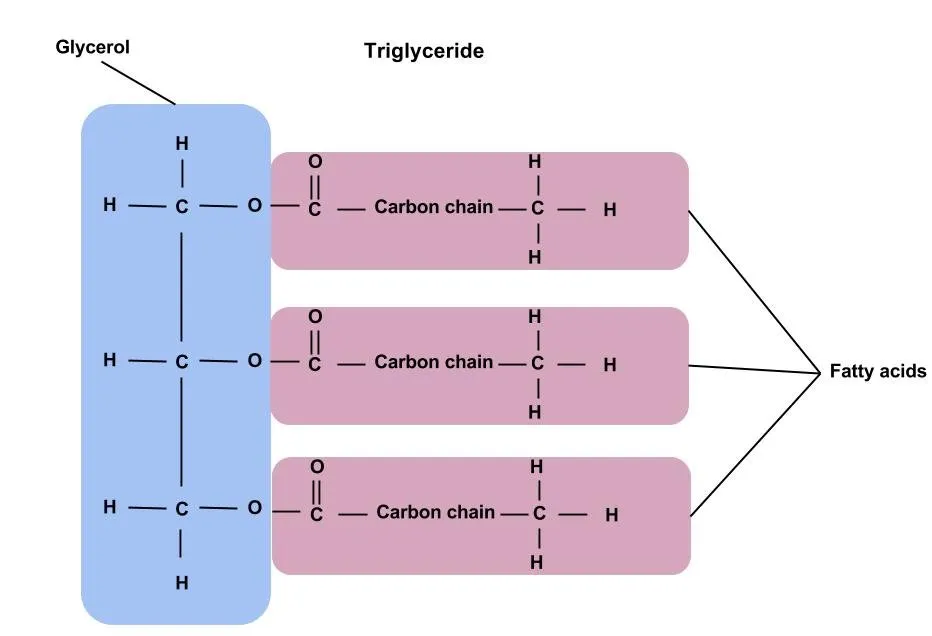
A triglyceride, as the name suggests, is built from a glycerol backbone plus three fatty acid chains. If all three of those chains are saturated fatty acids (i.e. only single carbon–carbon bonds), then that triglyceride is a fully saturated fat. But in real foods, many triglycerides are mixed — i.e. one or two saturated chains mixed with one unsaturated chain.
(Optional read) What about trans fat
Trans fat (or trans fatty acid) is a type of unsaturated fat that had its molecular structure altered (partially hydrogenated) so that the hydrogen atoms around a carbon–carbon C=C double bond sit on opposite sides—that’s what “trans” means.
Natural oils have cis-bonds instead, with hydrogen atoms on the same side.
(Optional read) Heating vs Hydrogenation
Heating oil in cooking will not add hydrogen — it may actually oxidize or break down the double bonds instead, forming aldehydes, peroxides, and other degradation products (the opposite of hydrogenation).
You can think of heating as damaging unsaturated bonds, while hydrogenation is chemically saturating them.
Why all of this matters
Saturated and trans fats both tend to raise LDL and apoB, while natural unsaturated fats (especially polyunsaturated ones) lower LDL and apoB.
Summary
- Cholesterol itself isn’t the villain—it’s an essential organic molecule our bodies make and need.
- Our liver produces most of it, while dietary cholesterol adds only a small fraction. Before that cholesterol even reaches your bloodstream, it must be digested, absorbed, and packaged to circulate the body.
- People vary in how much cholesterol they absorb—some are “hyper-responders,” but most absorb little, thanks to genetic and metabolic differences.
- The quality of fat in your diet shapes your cholesterol profile far more than the quantity of cholesterol in your food. Stay away from trans fat and limit closely saturated fats.
References
Cholesterol biology and absorption
(1) Ferrari A, et al. Science. 2023. “Aster-dependent non-vesicular movement of cholesterol from the plasma membrane to the ER downstream of NPC1L1.”
(2) Harman J. Nature Reviews Cardiology. 2024. “New insights into dietary cholesterol absorption.”
(3) Xiao J, et al. Nature Communications. 2023. “Bile acids facilitate intracellular cholesterol transport in enterocytes.”
(4) Nguyen TM, et al. Journal of Lipid Research. 2012. “ACAT2 is essential for efficient intestinal cholesterol absorption.”
(5) Long T, et al. Nature Communications. 2021. “Human ACAT2 structure and function in enterocytes and hepatocytes.”
(6) Shamir R, et al. Journal of Clinical Investigation. 1996. “Carboxyl-ester lipase hydrolyzes dietary cholesteryl esters, enabling absorption as free cholesterol.”
(7) Gilham D, et al. Journal of Biological Chemistry. 2007. “Pancreatic carboxyl ester lipase and dietary cholesterol hydrolysis.”
(8) Mokhtar FBA, et al. Atherosclerosis. 2022. “Roles of ABCG5/8 and NPC1L1 in cholesterol absorption and hepatic sterol flux.”
Inter-individual variability in absorption
(9) Lütjohann D. Biochimica et Biophysica Acta. 2019. “Fractional cholesterol absorption in humans: inter-individual variability and metabolic adaptation.”
(10) Mokhtar FBA. Atherosclerosis. 2022. “Genetic variation in ABCG5/8, NPC1L1, APOE, MTTP, and LDLR explains differences in dietary cholesterol responsiveness.”
(11) NCBI Bookshelf. (2024). Human Lipid Metabolism and Absorption Overview.
Dietary fat quality and cardiovascular effects
(12) Hooper L, et al. Cochrane Database Syst Rev. 2020;5:CD011737. “Reduction in saturated fat intake for cardiovascular disease.”
(13) Sacks FM, et al. Circulation. 2021. “Dietary fats and cardiovascular health: A Presidential Advisory from the American Heart Association.”
(14) Hart TL, et al. Journal of Clinical Lipidology. 2025. “Meta-analysis of polyunsaturated-to-saturated fat ratio and LDL-C change in controlled isoenergetic trials.”
(15) Mensink RP, et al. American Journal of Clinical Nutrition. 2003. “Effects of dietary fatty acids and carbohydrates on serum total-to-HDL cholesterol ratio.”
(16) Micha R, et al. BMJ. 2021. “Global, regional, and national consumption of trans fat and related health impacts.”
Trans fats and hydrogenation
(17) Mozaffarian D, et al. New England Journal of Medicine. 2006. “Trans fatty acids and cardiovascular disease.”
(18) Gunstone FD. European Journal of Lipid Science and Technology. 2021. “Hydrogenation of fats and oils: theory and practice.”
(19) U.S. Food and Drug Administration. Final Determination Regarding Partially Hydrogenated Oils. 2018.
(20) World Health Organization. Global elimination of industrially produced trans fat: 2023 progress report.
Mechanisms and physiology
(21) Ference BA, et al. European Heart Journal. 2017. “Low-density lipoproteins cause atherosclerotic cardiovascular disease: evidence from genetic, epidemiologic, and clinical studies.”
(22) Voight BF, et al. Lancet. 2012. “Plasma HDL cholesterol and risk of myocardial infarction: Mendelian randomisation analysis.”
(23) European Society of Cardiology / European Atherosclerosis Society (ESC/EAS). Focused Update. 2025.
(24) National Lipid Association (NLA). 2025 Clinical Practice Recommendations on Lipid Management.
(25) American Heart Association (AHA). 2022 ACC Expert Consensus Decision Pathway on Nonstatin Therapies for LDL-C Lowering.