How cholesterol moves in the blood – All About Cholesterol Part 2
How cholesterol actually travels through your blood — lipoproteins, apoB, and a ranked look at what genuinely lowers your cardiovascular risk.
In Part 1, I explained that cholesterol itself is not some foreign toxin invading the body.
Cholesterol is a normal, essential molecule. The problem is how it is packaged, transported, and, in some situations, deposited in places where it does not belong.
That brings us to the next obvious question: if cholesterol is so important, how does it move through the bloodstream in the first place?
It does not float around freely.
Cholesterol and triglycerides are largely water-insoluble, and blood is a water-based environment. So the body has to package these lipids into microscopic transport particles called lipoproteins. These particles have a lipid core and a surface made of phospholipids, free cholesterol, and specialized proteins called apolipoproteins. In other words, LDL, HDL, VLDL, and chylomicrons are not different kinds of cholesterol. They are different transport vehicles carrying lipid cargo through the circulation.
Table of Contents
Cholesterol is the cargo. Lipoproteins are the vehicles.
First of all, let’s understand what these letters mean.
- VLDL: Very Low Density Lipoprotein
- IDL: Intermediate Density Lipoprotein
- LDL: Low Density Lipoprotein
- HDL: High Density Lipoprotein
This is a video that I create with an easy to follow analogy.
▶ Watch on YouTube
For a more detailed explanation, see below. I will number the events because I understand that it is not so simple to picture what is happening.
- After a meal, the intestine packages dietary fat into chylomicrons.
- The liver, meanwhile, produces VLDL particles to export triglycerides and cholesterol made or processed by the body itself.
- As VLDL particles lose triglycerides in the circulation, they become IDL, and then eventually LDL.
- HDL participates in reverse cholesterol transport, helping move cholesterol from peripheral tissues back toward the liver.
- This is the simplified traffic map.
So when someone says they have “high cholesterol,” what they usually mean is that they have too much cholesterol being carried in one or more of these particles.
But clinically, the more important question is often not just how much cholesterol is being carried. It is how many potentially atherogenic particles are circulating.
That is where apoB enters the conversation.
ApoB is one of the most important concepts in lipidology
If you only remember one thing from this post, remember this:
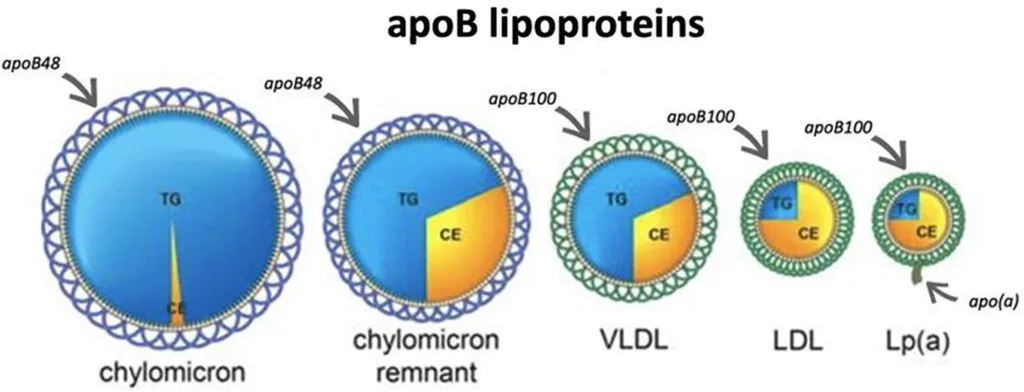
Every major atherogenic lipoprotein particle carries one apoB molecule.
That includes VLDL, IDL, LDL, and lipoprotein(a). Because there is essentially one apoB per particle, an apoB blood level works as a direct estimate of the total number of atherogenic particles in circulation.
Recent National Lipid Association guidance emphasizes that apoB more accurately reflects the atherogenic burden of lipoproteins than LDL-C alone.
This is why the old “good cholesterol versus bad cholesterol” story is too simplistic for serious risk assessment.
LDL-C tells you the mass of cholesterol inside LDL particles. ApoB tells you the number of atherogenic particles on the road.
Those are not the same thing.
Why LDL-C and apoB can tell different stories
Two people can have the exact same LDL-C and still have meaningfully different cardiovascular risk.
Why? Because LDL particles do not all carry the same amount of cholesterol. One person may carry a given amount of cholesterol in fewer, cholesterol-rich particles. Another may carry that same amount in many more, cholesterol-depleted particles. The second person has more particle traffic, more opportunities for arterial wall penetration, and potentially more risk.
A quick an simple example of same LDL-C and different Cardiovascular Risk
- Person A: Has 3 LDL particles with 5 cholesterol inside each particle. So the total LDL-C would be 3 x 5 = 15.
- Person B: Has 5 LDL particles with 3 cholesterol inside each particle. So the total LDL-C would be 5 x 3 = 15.
A 2024 analysis from the UK Biobank showed this problem clearly. At an LDL-C of about 130 mg/dL, 10-year ASCVD event rates were 7.3% versus 4.0% in people with higher versus lower apoB. In other words, the same LDL-C could conceal very different outcomes.
This becomes more relevant in people with insulin resistance, central adiposity, diabetes, metabolic syndrome, and hypertriglyceridemia, where cholesterol-depleted apoB particles are more common. But the discordance is not limited to obviously unhealthy patients. A 2024 JAMA Cardiology analysis found substantial apoB variability across the same LDL-C or non-HDL-C range even among metabolically healthy adults. That means a person can have a “decent” LDL-C and still be carrying more atherogenic particles than the lipid panel seems to suggest.
Non-HDL-C is all the cholesterol (cargo) inside all of the particles, except for the HDL particle. It is a better measure than LDL-C, but still does not tell us how many particles are circulating in the blood.
HDL is not a free pass
At this point, a lot of people ask: “Fine, but what about HDL? Isn’t that the good cholesterol?”
Not exactly.
HDL does participate in reverse cholesterol transport, and low HDL-C often travels with worse cardiometabolic health. But modern evidence has made the old HDL narrative much less convincing. Mendelian randomization studies and multiple failed HDL-raising drug trials have made it hard to argue that simply raising HDL-C, by itself, reliably reduces cardiovascular events. So while HDL biology is important, a high HDL-C should not be treated like a magic shield that cancels out a high apoB or a high burden of LDL-related risk.
Not only that, but a high HDL can mean dysfunctional particles that are causing even more harm.
Triglycerides matter too, but in a different way
Triglycerides are not cholesterol, and they are not interchangeable with apoB. But they still matter.
Elevated triglycerides often signal increased traffic in VLDL and remnant particles, which are also apoB-containing and potentially atherogenic. That is one reason triglycerides frequently are related with insulin resistance, fatty liver, abdominal obesity, and low HDL-C.
In these settings, relying only on LDL-C can underestimate risk, which is part of why non-HDL-C and apoB often provide more useful information than LDL-C alone.
LDL-C is often not measured directly.
It is calculated based on a formula that involves Total Cholesterol, HDL, and Triglycerides.
The problem is that as triglycerides rise, this calculation becomes increasingly inaccurate — sometimes giving a falsely reassuring number.
Takeaway
So what should you actually remember from all this?
- Cholesterol is the cargo, not the vehicle.
- LDL-C is not the same thing as particle number. It measures how much cholesterol is inside LDL particles, not how many atherogenic particles are circulating.
- ApoB is often a better representation of atherogenic burden, especially when triglycerides are elevated or when cardiometabolic dysfunction is present.
- If apoB is not available, non-HDL-C is often a more useful fallback than LDL-C alone because it captures cholesterol carried across all apoB-containing particles, not just LDL.
- Lp(a) will be discussed later, but it is important to know for now that current lipid guidance supports measuring it at least once in adulthood for most people, since it is largely genetically determined and can materially change risk assessment.
References
Core physiology and lipoprotein biology
(1) Feingold KR, et al. NCBI Bookshelf. 2023. “Introduction to Lipids and Lipoproteins.”
(2) Hussain MM, et al. Annual Review of Physiology. 2003. “Assembly and secretion of triglyceride-rich lipoproteins.”
(3) Ginsberg HN. Journal of Clinical Investigation. 1998. “New perspectives on atherogenesis: role of lipoproteins.”
(4) Goldberg IJ. Journal of Clinical Investigation. 1996. “Lipoprotein lipase and lipolysis.”
(5) Mahley RW, et al. Journal of Lipid Research. 1984. “Plasma lipoproteins: structure and function.”
ApoB as a marker of particle burden
(6) Langlois MR, et al. Current Cardiology Reports. 2020. “Non-HDL Cholesterol or apoB: Which to Prefer as a Target for the Prevention of Atherosclerotic Cardiovascular Disease?”
(7) Ference BA, et al. European Heart Journal. 2017. “Low-density lipoproteins cause atherosclerotic cardiovascular disease.”
(8) Walldius G, et al. Circulation. 2001. “Apolipoprotein B and apolipoprotein A-I: risk predictors of myocardial infarction.”
(9) National Lipid Association (NLA). 2024–2025. “Clinical recommendations on apoB and lipid measurement.”
Particle number vs cholesterol content
(10) Mora S, et al. Circulation. 2014. “Discordance between LDL cholesterol and particle number.”
(11) Ference BA, et al. JAMA Cardiology. 2020. “Association of discordance between apoB and LDL-C with cardiovascular risk.”
(12) UK Biobank investigators. European Heart Journal. 2024. “Apolipoprotein B and cardiovascular risk across LDL-C strata.”
HDL is not causally protective
(13) Voight BF, et al. Lancet. 2012. “Plasma HDL cholesterol and risk of myocardial infarction: Mendelian randomisation analysis.”
(14) Keene D, et al. BMJ. 2014. “Effect on cardiovascular risk of high density lipoprotein targeted drug treatments.”
(15) Rohatgi A, et al. New England Journal of Medicine. 2014. “HDL cholesterol efflux capacity and cardiovascular risk.”
Triglycerides, remnant particles and ASCVD risk
(16) Nordestgaard BG. Circulation Research. 2016. “Triglyceride-rich lipoproteins and atherosclerotic cardiovascular disease.”
(17) Varbo A, et al. Journal of the American College of Cardiology. 2013. “Remnant cholesterol and cardiovascular risk.”
(18) Toth PP, et al. Journal of the American College of Cardiology. 2021. “Triglyceride-rich lipoproteins, remnants, and cardiovascular disease.”
What to measure and why
(19) American Heart Association (AHA) / American College of Cardiology (ACC). 2022. “Expert Consensus Decision Pathway on Nonstatin Therapies.”
(20) European Society of Cardiology / European Atherosclerosis Society (ESC/EAS). 2025. “Guidelines for the management of dyslipidemias.”
(21) National Lipid Association (NLA). 2025. “Clinical Practice Recommendations on Lipid Management.”
(22) Mach F, et al. European Heart Journal. 2019. “ESC/EAS Guidelines for the management of dyslipidaemias.”
Lipoprotein(a) Genetics and risk
(23) Tsimikas S. Journal of the American College of Cardiology. 2017. “A test in context: Lipoprotein(a).”
(24) Kronenberg F. European Heart Journal. 2022. “Lipoprotein(a): current knowledge and future perspectives.”
(25) American Heart Association (AHA). 2023–2024 Scientific Statements. “Lipoprotein(a) and cardiovascular risk.”